|
|
|
Diagnosis and Management of Graves' Orbitopathy
with Standardized Echography 2.
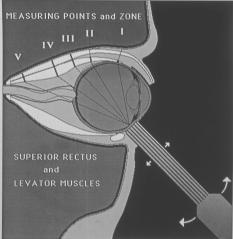
Measuring Points: A. Medial,
Superior and Lateral Rectus Muscles (Figs. 1,2,7 ):
These three muscles can be reliably measured and compared between
the two orbits of a patient and over 1)
INSERTING TENDON as
far foreward as possible (tendon pattern immediately following the
scleral signal (outer scleral surface spike and anterior (inner) tendon
surface spike are one and the same). 2)
TENDON HALFWAY BETWEEN INSERTION (1) AND MOST ANTERIOR
BELLY (3) 3)
MOST ANTERIOR MUSCLE BELLY:
as the beam
travels posteriorly, the muscle pattern not only widens but also shifts
away from the globe pattern toward the orbital bone signal.
The most posterior point
at which the maximized bone spike (muscle sheath surface spike next to
bone) is still maximally high, is the measuring point # 3, Any further angling of the beam in a posterior direction will
result in a drop of this (bone) surface spike from its 100% high
maximum. 4)
POINT OF MAXIMUM THICKNESS OF MUSCLE BELLY: this
is the only relative measuring point which will change according to type
of disease underlying a muscle thickening or thinning. Still, its comparison over time and with the corresponding
muscle in the fellow orbit is fully valid. 5)
APICAL (most
posterior) SEGMENT OF MUSCLE. Figure
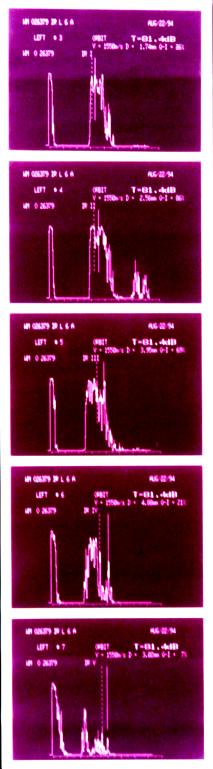
7:
Measurement of SR + Levator at 5
measuring points (left series) and of SR and Levator individually (left
and right echograms in right series)
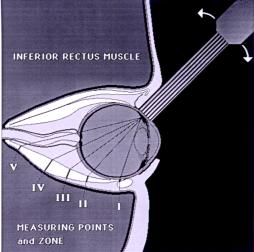
B.
Inferior Rectus Muscle
(Fig. 8):
This
muscle offers usually only 3
reliable measuring points: 1)
MOST ANTERIOR BELLY (behind
crossing of inferior oblique muscle).
There are two reasons why the inserting tendon of the inferior
rectus muscle can not always be measured: a)
the superior orbital rim prevents the probe to be pushed posteriorly
enough for the beam to reach the inserting tendon at a favorable angle.
Even raising of the patient's chin, which clearly improves the examination
condition for the inferior rectus muscle, does not ususally suffice to achieve above goal.
b) the over-lying
belly of the inferior oblique muscle is likely to interfere and confuse
the examiner about the true maximum thickness of the inferior rectus inserting tendon. 2)
POINT OF MAXIMUM THICKNESS
OF MUSCLE BELLY: the
reason why the #3 measuring
point of the other straight muscles is usually not applicable to the
inferior rectus muscle is that it often does not come to lie next to the
bony orbital floor. Rather,
it remains separated from the orbital floor throughout the orbit by
peripheral orbital fat tissue.
. 3)
APICAL (most
posterior) SEGMENT OF MUSCLE. Important: The
inferior rectus muscle crosses over the inferior orbital fissure in an
oblique fashion. The
inferior fissure, however, also
produces a pattern of decreased reflectivity simulated by the partial
blockage of the ultrasound beam at the level of the orbital floor (only
part of the beam enters the extraorbital tissues through the fissure and
weakened echoes from these tissues result).
Watch
out, not to confuse the fissure pattern
with the muscle pattern. Such
confusion can be avoided safely by (1)
considering that the IR lies more nasally than 6:00 and (2) by dynamically identifying the inferior
Figure 8: measuring
the inferior rectus muscle at the C.
Superior Oblique Muscle(Fig.
9): This muscle has 3 specific measuring points: 1)
INSERTING TENDON: this is the most important measuring
point of this muscle for the diagnosis of superior oblique myositis and
trochleitis. 2)
ANTERIOR BELLY OF MUSCLE (maximum
thickness behind the trochlea). Again,
this measuring point is important especially for the diagnosis of
myositis. 3) POSTERIOR BELLY OF MUSCLE (maximum thickness in posterior orbit and apex). This measuring point is particularly significant in the diagnosis and management of Graves'
orbitopathy. Figure
9: measuring a thickened (myositis) right superior
oblique muscle at 4 measuring points - I, III, IV, patient (right series)
D.
Inferior Oblique Muscle(Fig.
10): This muscle has 2 specific measuring points: 1)
MUSCLE BELLY (maximum thickness at or 2)
INSERTING TENDON
Figure
10 (right above): measuring a (myositic)
inferior oblique muscle at its two measuring points: I (top echoram) and
IV (bottom) 3.
MEASURING ACCURACY:
Using precise digital measurements
as offered by the MINI-A Scan Instrument, easy, quick and precise
as well as accurate
measure-ments of the straight and oblique extraocular muscles can be
performed by the trained echographer.
The measuring accuracy of Standardized Echography far surpasses
that of the radiological imaging methods.
Both the dynamic approach and the high resolution of echography
are responsible for this advantage of Standardized Echography.
The actual measuring accuracy depends on the muscle measured, the
measuring points used, and the disease process involved.
It is always better than
+- 0.3 mm. If a medial
or lateral rectus muscle is measured, and the muscle has low
reflectivity (e.g., in myositis) the measuring accuracy can be as good
as +- 0.1 mm, especially when the inserting tendon is measured.
When, on the other hand, the involved muscle is (1) the superior
rectus muscle, (2) has high reflectivity
(because of the disease process, e.g., Graves' orbitopathy), (3)
cannot be differentiated from the levator muscle (in the posterior orbit
where both are measured together), and (4) has irregular thickening
(often the case in Graves' orbitopathy), the measuring accuracy may be
as low as +- 0.3 mm. In
general, however, even under less favorable conditions, a difference of
> 0.5 mm between the two corresponding muscle bellies or a difference
of > 0.2 mm between the two correspon-ding inserting tendons in the
two orbits of a patient, is always dia-gnostic for muscle pathology. Important:
(1)
The comparison between right and left orbits is much more
meaningful and clinically significant than the absolute values (the
normal range of muscle thicknesses is wide and overlaps greatly the
abnormal range); in
contrast, the comparison between two correspon-ding muscles in the two
orbits of a patient is a highly sensitive indicator of wheter a muscle
is abnormal or normal.
(2) When the
measurements differ only slightly between the two orbits, repeated
measurements of the thinner muscle with the aim at getting a wider
measurement of this muscle and thus disproving thickening of the
previously wider measured muscle is an effective technique for avoiding
mistakes.
(3) Always measure
e.o. muscles with the patient's eyes in pri-mary gaze position.
If this is not possible, then compare the two orbits in strictly
symmetric gaze directions. III. Quantitative
A-Scan for the Diagnosis of Graves'Orbitopathy
About 60% of all cases of muscle disorders in the orbit are pa-tients
suffering from Graves' disease.
While these patients have a variety of abnormal orbital findings,
the thickening of the extraocular muscles is the key to the diagnosis. A.
Acoustic Criteria: ·
Bilateral
(often asymmetric) exophthalmus
(Hertel's readings corrected by axial eye length measurements) ·
Augmented
and coarsened orbital soft tissues
·
No
orbital mass lesion
except for slightly higher incidence of orbital "pseudotumor"
[pseudolymphomas,
granulomas] ·
Thickening of extraocular
muscles:
posterior, asymmetric
high-reflective irregular internal structure
variable over time
variable between corresponding muscles
OD / OS
myositic component of some muscles in 5%
of the cases ·
Thickening of optic nerve
sheaths ·
Thickening of periorbitae ·
Swelling (not
infiltration) of lacrimal
glands (asymmetric) B.
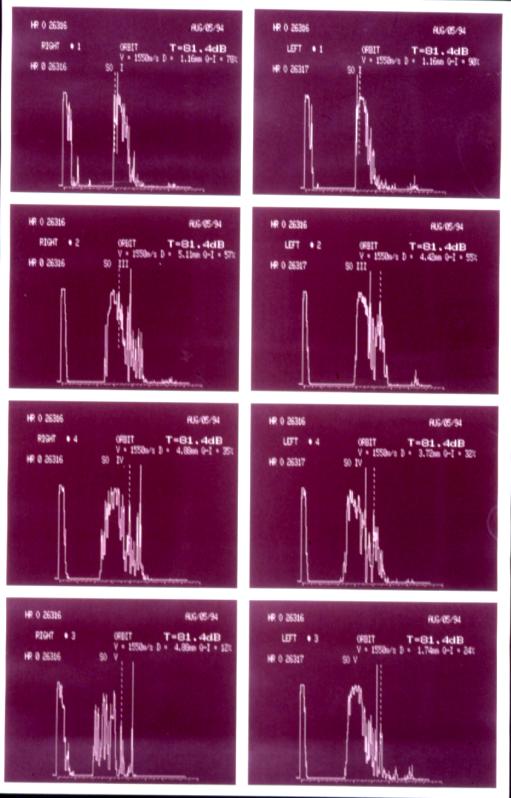
Acoustic Profile
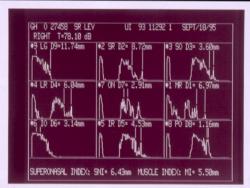
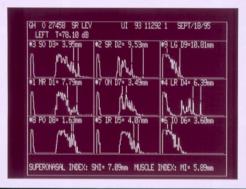
(Fig. 11): The maximum
thicknesses of all extraocular muscles together with the thicknesses of
the optic nerve sheaths, the periorbi-tae, and the lacrimal glands are
documented by mounting the echogra-phic pictures of these structures of
both orbits of a patient. The
acoustic profile is arranged according to the topography of the measured
struc-tures as one looks face to face at the patient.
The acoustic profile serves the purpose of
(1) grading the
severity of the Graves' orbitopathy,
(2) selecting cases that need more frequent follow-up and may be
endangered by compression of the optic nerve, and (3) following the natural course or the effectiveness of treatment
in a quantitative fashion. An important part of the acoustic
profile is:
Figure
11: documentation of orbital profile of right (left
group) and left (right group) orbital profile of a
C.
The Muscle Index (Fig. 12):
The
Muscle Index (MI) of an
orbit is the sum total of the maximum thicknesses of the 6 extraocular
muscles, divided by 6.
Normal MI:
< 5.0
Mild Graves' orbitopathy:
4.5 - 5.5
Grade I
Moderate Graves' orbitopathy:
5.5 - 6.5
Grade II
Severe Graves' orbitopathy:
> 6.5
Grade III
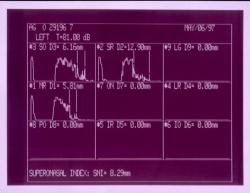
Another important part of the orbital
profile is the D.
Superonasal Index (Fig. 12): The
Superonasal Index (SNI) of an orbit is the sum total of the maximum
(most posterior) thicknesses of the medial rectus, the superir oblique
and the superior rectus muscles divided by 3.
Normal SNI:
<
5.75
Danger for ON compression
=>
7.0
Grade IV
Figure
12 (bottom left): documentation of left
SNI in patient with Grade IV Graves' orbitopathy. E.
Clinical Role of Standardized
Echography: ·
Diagnosis and Differential Diagnosis ·
Follow-up:
natural course
quantitative assessment of treatment. ·
Detection or Confirmation of active
CON
·
Grading
(see
also above): Grade I
mild
Follow-up elective
(MI) Grade II
moderate
Follow-up 1 - 1 1/2 years
(MI) Grade III
severe
Follow-up 1/2 - 1 year
(MI) Grade IV
CON threatened Follow-up
3-6 months months (SNI) Grade V
CON
Follow-up 6 weeks - 3 months
(Echo of ON) Grade VI
Functional Loss
Follow-up 2-4 weeks to confirm progression ®
surgery
|